|
第307回 東京レントゲンカンファレンス
2008年09月25日開催
|
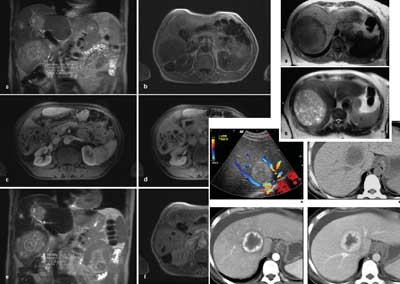
| 症例3 60歳代 男性 |
| |
|
経過補足
・前医では当初脂肪性肝炎が疑われていた。
施行されたエコー下生検では"sinusoidal dilatation"の結果であった。
肝腫大や汎血球減少の悪化があり、経過からPeliosis hepatisと診断された。
・病変は全肝に及んでおり、状態は急激に悪化しつつあった。
原因は明らかでなく、特発性と判断された。
以上から、肝移植を目的として当院に転院となっている。
・転院後はDICや静脈瘤の治療を行いつつ、全身状態の評価を進めた。
Child-Pugh scoreは12p (Grade C),MELD scoreは13pであった。
(三ヶ月間のmortalityは27%で、肝移植の適応と評価される)
・以上から、子をドナーとしたLDLT(Living Donor Liver Transplantation)を1ヶ月後に予定していた。
・しかし肝機能はさらに悪化し、熱発。
血液培養でグラム陰性桿菌肺炎が陽性となり、胸部単純写真で肺炎像が出現した。
・短時間のうちにARDSに移行し、全身状態が悪化。永眠された。
・同日、肝臓部分切除のみの剖検が施行された。
|
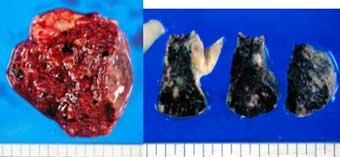
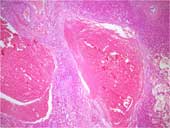
剖検肝 肉眼所見 組織像(HE x4)
 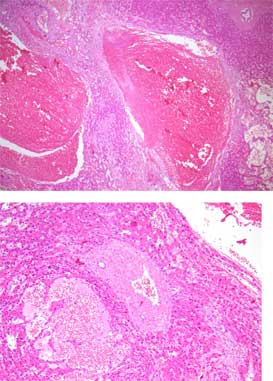 組織像(HE x10) 組織像(HE x10)
|
| |
Peliosis hepatis (hepatic peliosis)
・Peliosis Hepatis is an uncommon vascular condition characterized by
randomly distributed multiple blood-filled cavities.
Size of the cavities usually ranges between a few millimeters to 3cm in diameter.
・“Peliosis” is a term derived from the Greek pelios,
which means “dusky” or “purple” referring to the color of the liver parenchyma with peliosis.
・Often asymptomatic and therefore diagnosed incidentally at autopsy.
・In some instances, hepatomegaly, ascites,portal hypertension, cholestasis,
and hepatic failure may be present.
・Severe abdominal pain may result from rupture and intraperitoneal hemorrhage.
・Peliosis hepatis can occur at any age, usually develops in adults without regard to sex.
|
| |
Causatives of Peliosis hepatis
・The pathogenesis of peliosis hepatis is unknown.
There are several hypotheses, such as, it arise from sinusoidal epithelial damage, increased sinusoidal pressure due to obstruction in blood outflow from the liver, or hepatocellular necrosis.
・Associated conditions
Drugs
・Anabolic steroids, corticosteroids, oral contraseptives, azathioprine, tamoxifen, estrogen …
Diseases
・Chronic infections; Pulmonary tuberculosis, HIV infection …
・Bacillary peliosis; genus Bartonella (cat scratch disease)
・Hematologic disorders; Hodgkin’s disease, multiple myeloma
・Malignancy; hepatocellular carcinoma …
・Transplantation - immunoglobulin therapy;
azathioprine, cyclosporine …
especially renal transplantation.
It can be found in up to 20% patients
|
| |
Treatment, Natural history
・The natural course of peliosis hepatis is regression after drug withdrawal, cessation of steroid therapy,
or resolution of an associated infectious disease.
・In general, if untreated, peliosis hepatis may be rapidly fatal.
・Because of its potential complications, surgical resection of the involved liver parenchyma should always be considered.
・In rare circumstances partial resection of liver or transplant may be required.
|
| |
Gross pathologic appearance
・Multiple, irregularly shaped blood-filled hepatic cavities. The lesions typically involve the entire liver.
|
| |
Microscopic examination
・Phlecectatic type; rupture may follow the intrinsic weakness of the fibers of the endothelial wall
the blood-filled spaces are lined with endothelium and are associated with aneurysmal dilatation of the central vein.
・Palenchymal type; rupture associates with focal hepatocyte necrosis
The spaces have no endothelial lining and they usually are associated with haemorrhagic parenchymal necrosis.
・Some considers both pattern to be one process, initiated by focal necrosis of liver parenchyma observed in parenchymal type progressing into formation of fibrous wall and endothelial lining around hemorrhage of phebectatic type.
・Fibrosis, cirrhosis, regenerative nodules,
and thrombosis, calcification may also be seen.
|
| |
Imaging findings
・The imaging findings of peliosis hepatis are variable depending on the pathologic patterns of disease, various stages of the blood component of the lesions, and concomitant hepatic steatosis.
・「出血による腔形成+慢性肝障害」の組み合わせ
・出血腔の所見は非特異的だが、「血管モノっぽい」
・CT,MRI findings of focal peliosis hepatis are not specific.
・Absence of a mass effect is considered characteristic of a peliosis hepatis pseudotumor.
静脈が圧排されていたため術前診断を誤った,という報告もある
|
| |
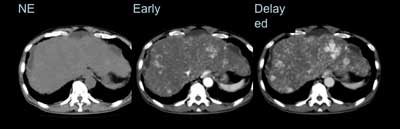
CT
・Peliotic lesions may be hyperattenuating to liver parenchyma.
・If peliotic cavities are smaller than 1 cm in diameter, CT findings may be normal.
・Calcifications within peliotic lesions have bee descrived.
・On contrast-enhanced CT, peliotic lesions can be hypoattenuating to liver parenchyma in the early acquisitions and tend to become progressively isoattenuating with time.
・Larger cavities communicating with sinusoids display the same attenuation of blood vessels.
・During the arterial phase of contrast enhancement,peliotic lesions typically show early vessel-like enhancement and multiple small accumulations of contrast material in the center of the lesions.
・During the portal venous phase, a centrifugal progression of enhancement without a mass effect on hepatic vessels is usually observed; a centripetal progression of enhancement can also be seen.
・On the delayed phase, late diffuse homogeneous hyperattenuation can also be seen.
|
| |
MRI
・The signal intensities of the lesions on MR examination
largely depend on the age and status of the blood component.
On T2WI, peliotic lesions are usually hyperintense to liver parenchyma with multiple foci of high signal, likely attributable to hemorrhagic necrosis.
On T1WI, the lesions are hypointense because of the presence of subacute blood, although isointense and hyperintense foci are also described.
On CE-T1WI, peliotic lesions usually show enhancement.
・Similar to CT, the enhancement is typically centrifugal
(from the center to the periphery of the lesion); however,
a recent report described an unusual centripetal enhancement pattern that may be confused with that of a hemangioma.
・Cystic cavities may reveal an enhancing rim that represents a hematoma.
・MRI with hepato-specific contrast agents seems to increase the diagnostic confidence, identifying hepatocytes and Kupffer cells within the lesion, but differentiation from hepatic adenoma with multiphasic CT or MRI is necessary.
|
|
US
・Conventional gray-scale sonography shows homogeneous hypoechoic lesions in patients with hepatic steatosis, hyperechoic lesions in patients with a healthy liver, and heterogeneously hypoechoic lesions if complicated by hemorrhage.
Doppler studies can show evidence of both perinodular and intranodular vascularity.
AG
・peliotic lesions appear as multiple vascular nodules during the late arterial phase.
・The enhancement of peliotic lesions typically is more distinct during the parenchymal phase and persists during the portal venous phase.
|
| |
Differential Diagnosis
・Vascular tumors
Hemangioma
・The typical enhancement pattern of hemangiomas is opposite of peliosis hepatis, and therefore differential diagnosis can be achieved in most patients.
Kaposi sarcoma, Angiosarcoma, Epithelioid endothelioma …
・Adenoma
may associated with estrogen. Presence of fat is useful sign to make DD. Focal peliosis can be
difficult to differentiate from adenoma.
・Hypervascular metastases, HCC, …
|
| |
この症例に立ち返ってみると…
・脂肪浸潤を伴う強い肝腫大、慢性肝障害パターンがある。
造影CTにて、主にcentrifugalな濃染を示す病変が多発している(血管系っぽい)。
MRIはいまひとつ決め手に欠けるが、HCCなどの広範な拡がりは否定的と考えられる。
・病理所見は典型的で、画像所見に反映されていると考えられる。
臨床経過も特発性肝紫斑病として矛盾がない。
・典型的な原因(薬剤や背景疾患)がないため、画像診断で診断を絞り込むことは難しかったと思われる。
・しかしもう少し早い時点で本疾患を鑑別に挙げ、矛盾がない生検結果を得られていれば、
移植までは可能であったかもしれない。
・まずは、本症の代表的な原因を念頭に置いておくことが重要かと思われます。
|
| |
|
| |
症例提示ページへ
|
|
|
|
|
|